
Ideas & TheoriesThis page contains descriptions for the mechanisms of change that catalyze client transformation and the helping and hindering forces that moderate and mediate the processes of outdoor therapies. |
MECHANISMS OF CHANGEMechanisms of change explain how these forms of outdoor therapy combine risk taking, conflict resolution, nature immersion, and intentional psychotherapy to transform clients behaviors, thoughts, and feelings. These theories are generalized and in need of hypothesis testing. Obviously, each type of program will blend these mechanisms in differing amounts. CHALLENGEThe principal mechanism of change for adventure therapy programs (overcoming risk and conflict challenges in small groups) is diagrammed below. The engine for this process is a repeating cycle of Distressful Dissonance, Attempt at Resolution, (if successful) New Found Competence, and Facilitated Reflection. Typically, these four are arranged in a sequential cycle, however, advanced practitioners are capable of mixing and matching these so each can occur at any point and in any order (even simultaneously) within the therapy. This meta-theory is explained with two relationships examples: intrapersonal (risk taking) and interpersonal (conflict resolution). |
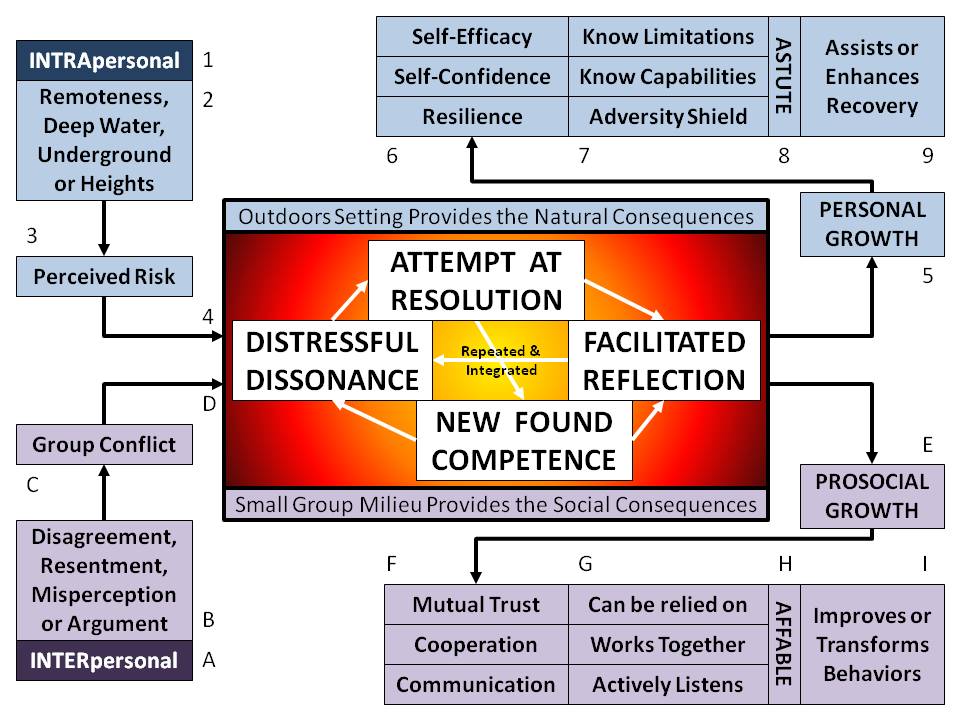 |
RISK TAKING: Psychological Self (Intrapersonal)In the psychological INTRApersonal relationship sequence (1), adventure therapists seek out conditions that most people fear (2): remote isolation (wilderness), fast/deep water (white water or ocean paddling), dark underground (caving), and heights (climbing or challenge courses). These unfamiliar exposures present the appearance of a high perceived risk (while real dangers are actually kept quite low by competent outdoor leaders) and the clients experience a fear response (3). In their minds, they have trouble reconciling two disparate extremes: "I’m safe and I’m going to die!" (4) This dissonance is distressful, so they attempt to resolve the situation by applying their personal skills and behaviours against the risk. If successful, they gain new competence and facilitated reflection helps them understand their growth with questions like: "what did you learn, where does that apply in your life, and what will you do differently next time or when you leave the program?" This cycle repeats, with the outdoor setting providing natural consequences, until personal growth results (5). Depending on the activity, therapy program, and its duration, location or intensity, this personal growth can have dozens of different outcomes, but at least three are common and worth following further: self-efficacy, confidence, and resilience (6). These respectively indicate clients who know their limitations and capabilities, while holding a shield against future adversity (7) and in combination these three characteristics make for astute individuals (8) who will use personal growth to assist or enhance their recoveries and prevent further relapses (9).  CONFLICT RESOLUTION: Social Self (Interpersonal)In the social INTERpersonal relationship sequence (A), adventure therapists wait for inevitable disagreements (navigation decisions), resentments (who impedes progress), misperceptions (favouritism), and arguments (unequal food portions) that often arise in small groups (B) under stress during outdoor living and ultimately lead to conflict (C). Again, the dissonance is distressful: “I have to be a team player, but I am so ready to settle this with agression!” (D) Under the guidance of the adventure therapist (present to also prevent violent escalation), the clients attempt to resolve the conflict by practicing their social skills and behaviours. If successful, they gain new competence and facilitated reflection helps them understand their growth with the same questions: “what did you learn, where does that apply in your life, and what will you do differently next time or when your leave the program?” Once more, the cycle repeats, with the small group milieu giving social rewards and penalties, until prosocial growth results (E). Depending on the activity, therapy program, and its duration, location or intensity, this prosocial growth can have a myriad of various results, but at least three are common and worth discussing further: mutual trust, cooperation, and communication (F). These respectively indicate clients who can be relied on, work well together with others, while actively listening to differing opinions (G) and in combination these three qualities make for affable individuals (H) who will use prosocial growth to improve or transform their societal behaviours going forward (I). |
NATURE IMMERSIONThe principal mechanism of change for nature or eco-therapy programs (focused on sensorily immersing individual clients in the restorative properties of nature) is diagrammed below. One fundamental tenet of conventional psychology is that unaddressed negative emotions can lead to diminished physical and mental health. Negative or antagonistic emotions might include anger, guilt, sadness, grief, loneliness, disgust, failure, resentment, apprehension, jealousy, and helplessness. The main premise of this form of eco-therapy is that exposure to nature brings a positive emotional outlook that can lead to healing, well-being, and enhanced physical and mental health. Examples of positive or affirmative emotions might be: joy, happiness, serenity, tranquility, peacefulness, hope, amazement, awe, admiration, inspiration, and appreciation of beauty. These can be accessed and accentuated by immersing the client in sensory awareness of a natural environment. This immersion is followed by a traditional talk therapy to clarify and cement change, while depending on the restorative properties of nature. The metaphor of a flower is used to describe this process of simply replacing negative emotions with positive ones inspired by nature. |
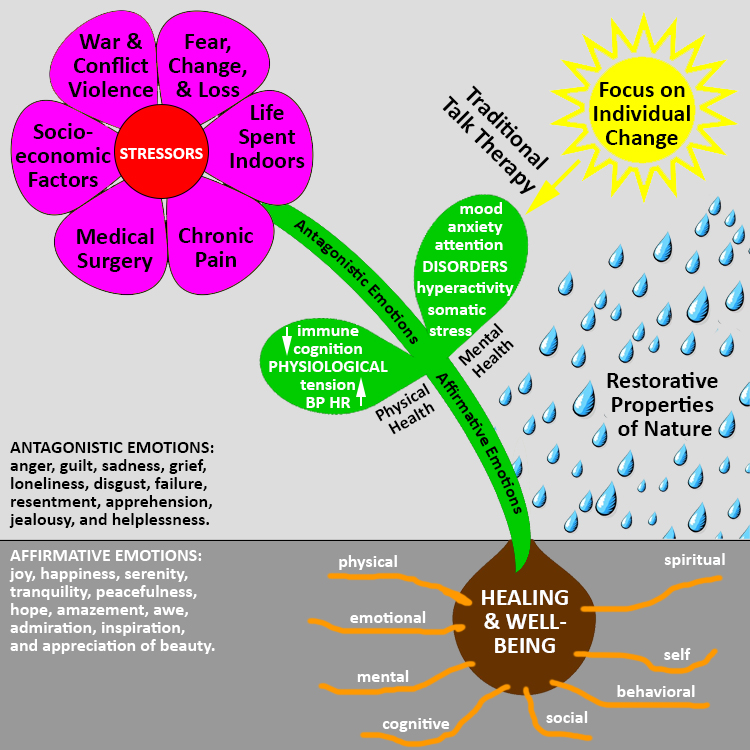 |
FlowerLife is full of stressors, including many minor ones which humans can easily cope with. However, some major ones leave a lasting influence. Surviving war or conflict violence, ultimately leads to post traumatic stress disorder. Living with poverty, food insecurity, homelessness, unemployment, and other socio-economic factors can govern a lifetime of fighting with friends and family. Recovering from medical surgery or living with daily chronic pain may diminish concentration, increase insomnia, and cause fatigue or irritability. Even a life lived indoors with artificial light, conditioned air, and controlled temperatures can directly alter health such as a deficiency in Vitamin D or an abundance of adrenaline and cortisone. Other major stressors include: the death of a loved one, marriage, divorce, separation, incarceration, job loss, retirement, work difficulties, accident, illness, injury, financial trouble, natural disaster, victim of crime or violence, and moving house. Stem & LeavesAll of these stressors cause a flood of negative or antagonistic emotions that are known to impact physical and mental health. These negatives substantiate disarray in feelings, thoughts or behaviors with the subsequent development of mood, anxiety, attention, hyperactivity, somatic, and stress disorders. Closely associated with these disorders are common physiological impacts of elevated muscle tension, blood pressure, and heart rate, with suppressed cognition and immune response. Psychological & Spiritual SelfJust as the animal-human bond potentiates equine and canine therapies, the spiritual connection between humans and nature drives the influence of eco-therapies based in forest, jungle, bush, parks, or other kinds of natural settings. Nature provides the restorative properties and positive feelings that wash away the negative feelings and cleanse the damages. A focus on individual change through traditional talk therapies addresses the mental health disorders which in turn treat the physical health symptoms and physiological indicators. Affirmative emotions arise from sensory immersion in nature and replace the antagonistic emotions, thus leading toward healing and well-being. Nature nourishes the soul and feeds the spiritual healing and well-being of the client. Bulb & RootsHealing and well-being are grounded to nature, where health is not the absence of disease, disorder, or infirmity, but the presence of physical, emotional, mental, cognitive, social, behavioral, self, and spiritual well-being. As an example, in land-based healing, an indigenous approach to wellness in Canada, people dispossessed from their ancestral lands return to those territories to follow traditional practices with cultural knowledge and elder story telling. They heal themselves from the trauma of forced dispossession by spiritually reconnecting with nature. |
INTENTIONAL PSYCHOTHERAPYThe principal mechanism of change for psychotherapy is talk. Talking about feelings, thoughts, and behaviours, rather than holding everything inside, can help people to better cope with problems, stress, troubles, worry, and difficulty. By “talking it out,” humans are able to determine what bothers them, develop solutions, and then calm down and relax. Shared talking builds new relationships, strengthens existing ones, and lets a person know they are cared about by others. The aim of psychotherapy is to assist clients in dealing with their potentially harmful feelings, thoughts or behaviors, and replacing these with healthy and effective feelings, thoughts, or behaviors that they can use to cope with their current concerns and future problems that may arise. Grounded in dialogue (to explore and understand the issues without deciding or passing judgment) and discussion (to confirm a course of action toward change and transformation), psychotherapy is typically conducted in a comfortable office setting. Confidentiality is guaranteed (except for certain disclosures of illegal intent or harm from a client) and the therapist remains objective, unbiased, and impartial. Established ground rules make sure the sharing is conducted in a climate of privacy and support. |
 |
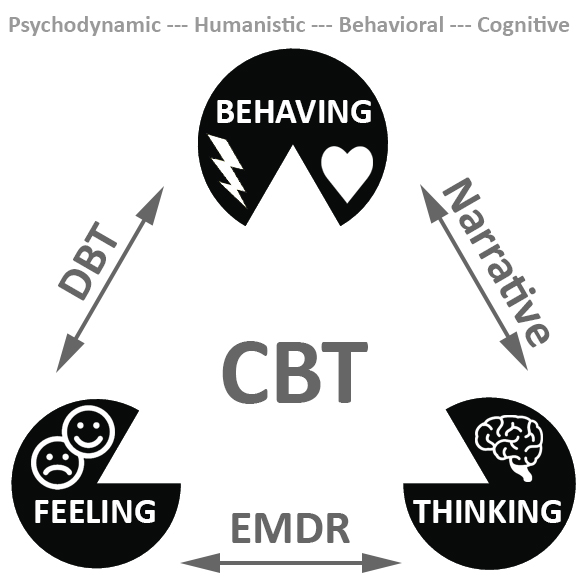
Traditional Talk TherapyTraditional talk therapies depend on the relationship congruency between client and therapist or among clients and therapeutic modalities (see hindering forces below). When these are misaligned, therapy can fail. The modalities used by a therapist are: often informed by research, a likely strength of the therapist, and hopefully custom modified for each client. The therapist may rely on a combination of talk therapy modalities and vary these to better suit each of the clients as more is learned about their particular issues. Here are descriptions of the philosphical schools of psychological thought and several therapy techniques evolving from these (as diagrammed below).
|
 |
ModalitiesMODALITIES commonly used by Canadian outdoor therapy programs
Also commonly being used in outdoor therapy within Canada are other modalities including:
|
HELPING & HINDERING FORCESBeyond the contributions to outdoor therapies of challenge, nature immersion, and intentional psychotherapy, four helping forces (positive, black arrows) and four hindering forces (negative, white arrows) are constantly at work on the viability of a client's therapeutic change. These eight are shown in the diagram below and described afterward. |
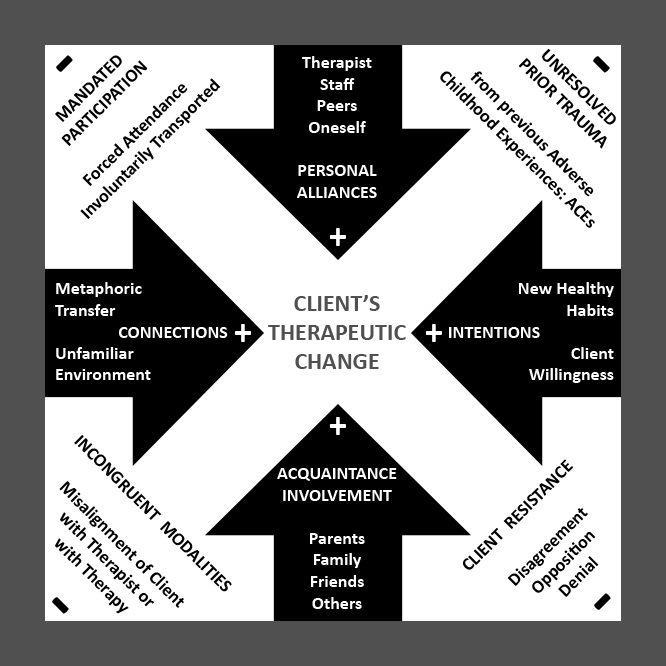 |
HelpingFOUR HELPING FORCES THAT CONTRIBUTE TO CLIENT CHANGE (+)
HinderingFOUR HINDERING FORCES THAT DETRACT FROM CLIENT CHANGE (-)
 |




