Best Practices
This page describe the indications (reasons for engagement) and contraindications (concerns against engagement) for outdoor therapies, separated by challenge and nature components. Safety and quality of programs are discussed in terms of risk management practices and questions to ask providers. We then list the providers of programs in Canada (without endorsement of any) and international organizations associated with outdoor therapies. Last, we share state-of-the-art facilitation techniques and framing (with metaphor) methods for consideration by therapists and non-therapists alike. |
INDICATIONS & CONTRAINDICATIONS
The greatest impact of outdoor therapies (also aided by traditional talk therapies with accompanying partners, families, or within small treatment groups) can be achieved with individual clients, who have not had success with other mainstream therapies. As primary therapy, adjunctive, or enriching treatment, outdoor therapies serve a combination of children, teenagers, and adults, who commonly present with one or more types of physical or mental health disorders and who can benefit from a combination of CHALLENGE (risk taking with conflict resolution in small groups) and individual immersion in NATURE. The following lists of indications and contraindications overlap and are by no means absolute. |
CHALLENGE
Indicated
- Substance use disorders
- Impulse control disorders
- Behavioral disorders
- Eating disorders
- Personality disorders
- Violence (perpetrators and survivors)
- Criminal (pre-release or post delinquent)
- Attachment issues
- Psychosis or Schizophrenia
|
CHALLENGE
Contraindicated
- Periculophobia (dangers)
- Anthropophobia (groups)
- Autophobia (being alone)
- Achluophobia (dark)
- Acrophobia (heights)
- Hydrophobia (water)
- Chionophobia (snow)
- Claustrophobia (feeling trapped in confined spaces)
|
NATURE
Indicated
- Anxiety disorders
- Mood disorders
- Stress disorders
- Somatic disorders
- Attention disorders
- Hyperactivity disorders
- Cognitive impairment
- Pain reduction
- Surgical recovery
|
NATURE
Contraindicated
- Biophobia (outdoors)
- Anthrophobia (flowers)
- Dendrophobia (trees)
- Entomophobia (insects)
- Zoophobia (animals)
- Heliophobia (sun)
- Astraphobia (lightning and thunderstorms)
- Agoraphobia (feeling trapped in open spaces)
|
Also generally indicated to benefit include:
- troubled teenagers impacted by peer pressure or socio-economic factors,
- accident survivors,
- refugees or migrants,
- children under protective services,
- absent or underperforming school students,
- youth disconnected from culture or community,
- adults needing respite from chronic or terminal disease,
- palliative care patients, and
- wounded service members.
|
Also generally contraindicated are those with:
- uncontrolled or severe disorders (especially arson/pyromania and unremorseful violence),
- obesity or lack of fitness (including poor cardiovascular health),
- major injuries that prevent movement or locomotion,
and those who are:
- undergoing medical treatment,
- taking certain prescription medications, and
- daily non-functional due to an over-reliance on others (parents) or sincerely suicidal (more than ideation).
|
|
SAFETY & QUALITY
Outdoor therapy programs have common concerns for safety and quality. General agreement exists that quality programs depend upon suitable risk management policies and procedures, competent practitioners (appropriately prepared in several competency sets), and the support of clients in achieving their therapeutic goals.
Risk management content ranges from primary (proactive procedures to prevent accidents), through secondary (active response to accident with own resources), to tertiary (reactive assistance from outside agencies) and other procedures. Risk management refers to carefully controlling real dangers at low levels (nothing can be 100% safe), while allowing clients to perceive and encounter high risks for therapeutic benefit in adventurous outdoor therapies. Despite the appearance that some of the adventure activities may be dangerous, actuarial data suggest that these activities are quite safe. Decades of data collection indicate that risky adventure activities are actually on par with daily living and have lower injury rates than traditional youth sports. Clients in legitimate programs were three times less likely to go to an emergency room for an injury in the field than at home. The average client participating in recreational sports was four times more likely to visit a hospital emergency room for an injury than from participating in outdoor therapy.
Competent practitioners are those who hold several desired characteristics (self-awareness, prosocial skills, ethics, resilience, traits, etc.) and exhibit praxis in three competency sets: the activities, reflection, and clientele. Activity competencies include the technical, risk management, safety, environmental, organizational, instructional, and meta skills of leadership. While not needing to be cross trained in all activities, they at least have a cushion of competence above that of the clients and are comfortable in a leadership role for the activities they choose to employ. They hold a skills certificate and insurance for each activity that legally requires so. Reflection competencies include psychotherapy modalities, facilitation techniques, the conscious use of metaphor, and trauma-informed care. Clientele includes understanding the issues, concerns, culture, indications and contraindications of clients and how to tailor activities and reflection to suit those needs. Practitioners have an appropriate level of first aid that matches the remoteness they work in. They are able to manage physical, socio-emotional, and behavioral concerns, and receive regular supervision from a qualified professional. Quality organizations are well versed in trauma-informed care, with sufficient client knowledge to provide culturally appropriate programming. Competent practitioners have an appropriate level of education and/or licensure for the services they provide. They follow the relevant ethical practices within their disciplines to enable goal attainment.
Therapeutic goals are being met with success. The volumes of research on outdoor therapies have been considerable for the past decade, with several meta-analyses indicating moderate treatment effect sizes for improvements in: self-efficacy, initial mental health status, self-concept, locus of control, pro-social behaviors, self-esteem, behavioral observations, personal effectiveness, clinical measures, recidivism rates, positive behaviors, academics, family development, and social development. Meta-analyses about immersion in nature have demonstrated similar improvements for nature connectedness, happiness, life satisfaction, well-being, and treatments of mental health disorders. Therefore, outdoor therapies support client outcomes more or less in line with other therapeutic modalities. A meta-analysis of regular time spent in greenspace showed clear physiological health benefits such as diminished cholesterol, cortisol (stress-related hormones), heart rate, blood pressure, heart rate variability (relaxation indicators). These benefits were linked to reduced chance of type II diabetes, stroke, general mortality, asthma, hypertension, and coronary heart disease. The majority of these outcome studies have been based on pre-post analysis of scores on psychometric instruments measuring symptom severity in clients.
Outdoor therapy programs have a clear mission. They identify the clients they serve effectively and those that would benefit from a different provider. They clearly indicate how they work with clients through treatment plans, therapeutic modalities, curriculum, activities or interventions, risk management plans, timelines, and expected outcomes. They describe in detail how they monitor ongoing client progress with information from multiple sources using appropriate assessment tools. Quality programs seek informed consent for participation from clients and have a defined process for them to leave treatment should they choose to. Operating in the clients’ best interests, quality programs ensure staff are adequately trained to provide effective treatment, ethically and culturally appropriate service, and transparent communications to client families. These programs track and report incidents and follow appropriate local regulations for operations, food services, clinical services, and transportation.
In an effort to improve program safety and quality by taking a holistic view of both, the international Association for Experiential Education has offered an outdoor program accreditation system since 1994. “Attaining accredited status … is solid evidence of an organization’s commitment to quality and safety, belief in professional standards, and allocation of resources toward continued excellence and improvement. Programs that achieve AEE Accredited status can be confident that they meet or exceed recognized industry standards.” A specialized accreditation for outdoor behavioral healthcare, wilderness, and adventure therapy programs was added in 2013 with clearly defined benchmarks for program quality and risk management practices. Finally, a recently developed credential for licensed mental health professionals to qualify as clinical adventure therapists has provided benchmarks for those in private practice. |
CANADIAN PROGRAMS
COMING SOON! We are still compiling this list. If you would like to have your program listed here alphabetically with a link to your website, please contact the coordinator below. PLEASE LET THEM KNOW YOU FOUND THEM ON C.O.T.H. Thanks.
This service is for therapy programs only. We do not list recreational, educational, or developmental programs. Cheers.
PROVINCE / TERRITORY |
RISK, Adventure / Wilderness Therapy, Outdoor Behavioral Healthcare, etc. |
INDIGENOUS, Land-based Healing (with or without Travel), etc. |
NATURE, Forest, Nature-based, Eco-therapy, etc. |
Canada-wide |
|
|
|
AB (Alberta) |
|
|
|
BC (British Columbia) |
|
|
|
MB (Manitoba) |
|
|
|
NB (New Brunswick) |
|
|
|
NL (Newfoundland & Labrador) |
|
|
|
NS (Nova Scotia) |
|
|
|
NT (Northwest Territories) |
|
|
|
NU (Nunavut) |
|
|
|
ON (Ontario |
|
|
|
PE (Prince Edward Island) |
|
|
|
QC (Quebec) |
|
|
|
SK (Saskatchewan) |
|
|
|
YT (Yukon Territory) |
|
|
|
|
INTERNATIONAL ORGANIZATIONS
CHALLENGE: Adventure/Wilderness/Outdoor Behavioral |
NATURE: Bush/Forest/Nature-based/Ecotherapy |
|
|
|
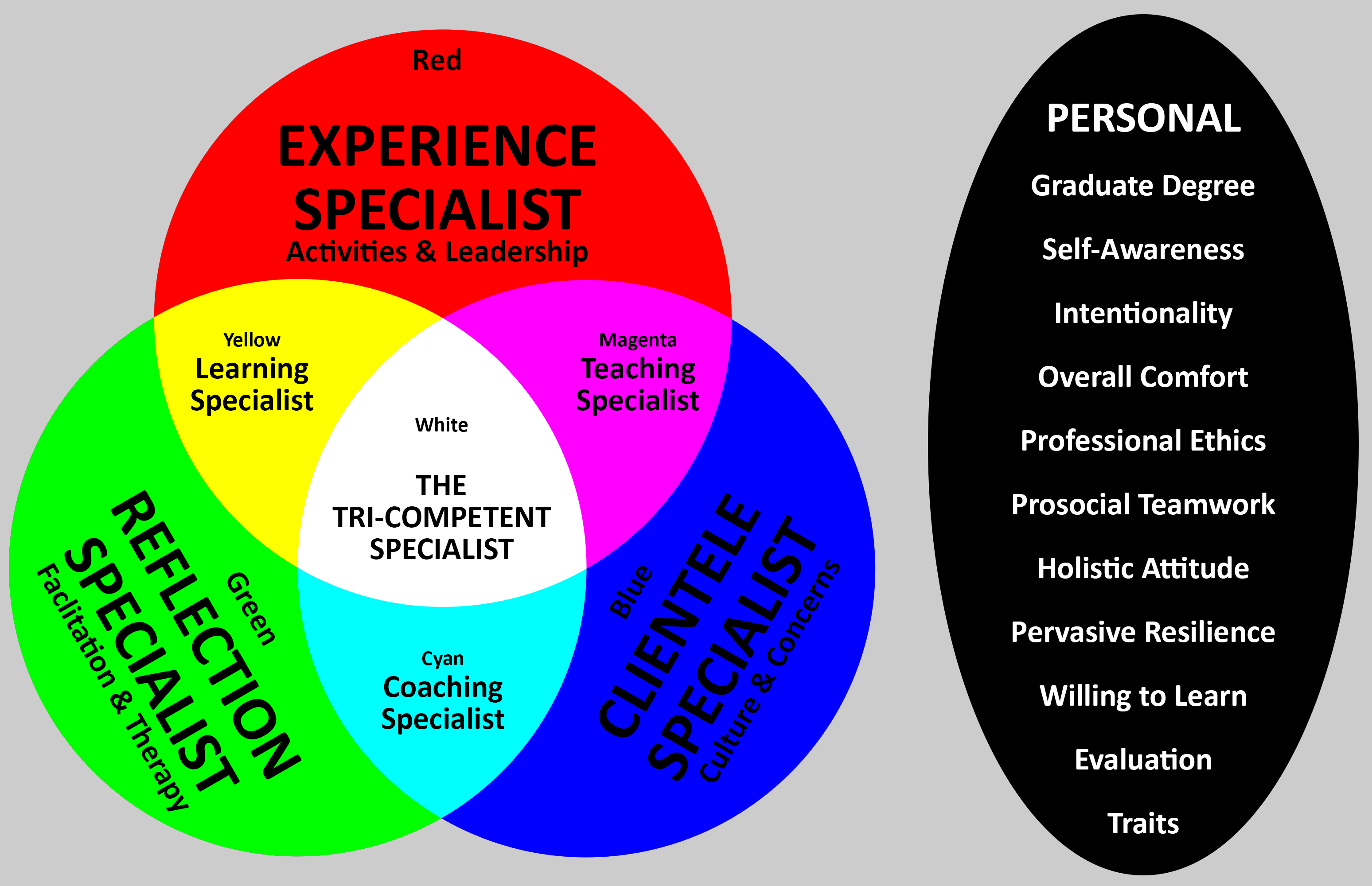
TRI-COMPETENCE
As diagrammed below, the successful outdoor therapy program requires staff with competence in three sets:
- the EXPERIENCES or leadership of the activities used with clients (red circle),
- the REFLECTION techniques employed to help them learn or change (green circle), and
- the precise needs and specific issues of the CLIENTELE themselves (blue circle).
The tri-competent specialist (white) is someone who has knowledge and ability in all three of these sets. However, the “tri-comp” is a rare beast and so a program must ensure that they cover all three of these competency sets in a combination of two or more staff (yellow, magenta, cyan). In addition, successful outdoor therapists also possess certain PERSONAL characteristics (black oval).
|
FACILITATION
 |
Facilitation means to make growth easier and is about non-therapy techniques. This includes anything the facilitators (outdoor leaders, group counselors, or community elders representating the therapist or the therapists themselves) do before, during, and after the challenge or nature immersion experience to assist the clients in learning and/or changing more effectively.
In the next table, facilitation techniques are arranged on the basis of complexity and difficulty across 4 types of outdoor programs and their primarily intended changes:
- Recreation (changes the way people FEEL),
- Education (changes the way people THINK),
- Development (changes the way they BEHAVE), and
- Therapy (changes the way they RESIST CHANGE).
Practitioners ought to be competent in the techniques listed for their type of programs, but also in those for the columns to the left. |
PROGRAM TYPE |
Recreation (FEELING) |
Education (THINKING) |
Development (BEHAVING) |
Therapy (RESISTING) |
FACILITATION TECHNIQUES |
NONE (the experience speaks for itself to entertain and enable feelings of joy and happiness) |
FUNDAMENTALS (organizing for unsequenced discussion with a few simple questions)
FUNNELLING (asking a sequence of questions after the experience to distill specific changes) |
FREEZING (stopping the action with a time out to ask a single provocative question)
FRONTLOADING (asking one or two questions before the experience to center attention on change within the experience) |
FORTIFYING (a stepwise order of techniques designed to strengthen against resistance)
FOCUSING (shifting the emphasis away from the problem and on to solutions) |
Fundamentals
Fundamentals refers to the basics of facilitating an unstructured group discussion by asking a minimum of three open-ended questions (what? so what? now what?) in a sharing circle.
Circles are good because they are warm and inviting, offer excellent hearing and eye contact, and allow for the observation of body language.
In these circles, people take turns speaking and have the right to pass and have their disclosures remain confidential.
Since this basic technique is an unstructured form of questioning, it lends itself best to exploring and confirming client issues.
Aside from ethical considerations, know why and what you are facilitating with respect to the program purpose and clients' needs.
Stay neutral and avoid taking sides or getting drawn into group conflict by clearly knowing your own values and triggers.
DO: discuss group process and not outcomes, allow enough time for discussion, balance doing & talking, make debriefs recent, proximal to the experience, and free of distractions.
DON’T: answer for clients, worry about right answers, compare clients to others, judge performance, offer false feedback, assume you know best, or focus on the negatives too early in the process.
Funnelling
Funnelling involves asking six structured and sequenced questions in sharing circles:
- Replay (used to remind clients of the past when the experience was not immediately recent) - Can you review the last experience for me?
- Remember (used to identify a good or bad example of the topic being discussed) - Do you recall a particulat time when __[topic]__ was excellent (poor)?
- Affect/Effect (used to discover the influence of the example) - How did that event impact you personally (the group and/or the task)?
- Summation (used to identify the lessons learned from the above) - How would you summarize your learning from our discussions?
- Application (used to metaphorically connect the experience to daily living) - Do you see any parallels between this learning and your life (at school, work, or home)?
- Commitment (used to pledge future changes) - What will you do differently in the next experience (or when you return to you daily life)?
Since this technique is a structured form of questioning, it lends itself best to enabling clients to change their thoughts (and feelings).
Freezing
When clients appear to be “stuck in a rut” and unable to extricate themselves, simply call a time-out to freeze the action and ask a single provocative question (How is your communication right now?), then return to the action as soon as possible.
Frontloading
Asking one or two questions, from this list of six types, immediately before the experience begins, so as to turn clients atention toward change.
- Revisiting (used to remind clients of past commitments) - Remind me; what were you going to do differently this time?
- Motivation (used to metaphorically connect clients to their daily lives in advance) - Where might learning from this experience be useful in the future?
- Objectives (used to identify lessons to be learned) - What do you think you will get from participating in this experience?
- Function (used to discover what is already being done well) - What will you need to succeed and how can we make sure that happens?
- Dysfunction (used to avoid failure or setbacks) - What has held you back in the past and how do we make sure that doesn't occur now?
- Prediction (used to orient clients toward a particular behavior or expectation) - What do you think is going to happen next in this experience?
Since this technique provides a reminder that centers attention immediately before engaging in the experiences, it lends itself best to enabling clients to change their behaviours (plus thoughts and feelings) during the experience and provide a direct comparison to their past behaviours.
Fortifying
This stepwise sequence of six psychotherapeutic techniques is aimed at bringing client transformation, when they are clinically resistant to change. Try the least intrusive method first and, if it fails, then progress to the next step.
- Client is Unaware of the change (use CLARIFICATION technique) - Have an admired friend or peer (not the facilitator) explain the change.
- Client is Unwilling to change (use NEGOTIATION) - Make a contract around what is needed to accomplish the change, then get those resources.
- Client is in Disagreement with the change (use CONFUSION technique) - Genuinely and respectfully ask the client to help you understand.
- Client is Unconsciously Opposing change (use PARADOX) - Behave unexpectedly from usual, in a reverent version of reverse psychology.
- Client is Consciously Opposing change (use Double Bind) - Describe two options going forward and ensure both are in the client's best interest.
- Client is Apathetic toward change (use ROLE SHIFT) - Find another perspective, position, or opportunity for each client, before removing them.
Ultimately, this form of treatment does not work for every single client and some may need to be referred to an alternative situation.
Focusing
Focusing refers to where the client's awareness and the facilitator's attention are directed. Both can center on the problem that presents or solutions that are not directly related to the problem and so are more welcomed as change by resistant clients. Here are the differences.
PROBLEM FOCUS |
SOLUTION FOCUS |
- Centers on reducing problems
- Looks at what clients are doing wrong and incorrectly
- emphasizes what they don't want
- Highlights what must be done better
- Seeks to eliminate weaknesses
- Interested in WHY the problem happens (what causes and sustains it?)
|
- Centers on enhancing solutions
- Looks at what clients are doing right and correctly
- Emphasizes what they do want
- Highlights what is already being done well
- Seeks to accentuate strengths
- Interested in WHEN the problem doesn't occur (what exceptions exist?)
|
A solution-focused facilitator is not simply sugar coating or pointing out the positives. This strength-based approach requires a philosophical shift and rewording of questions. Consider these three examples.
AFTER (funneling): On a scale from 0-low to 10 high, how was your ________ in this activity?
- Problem = What will you need to do to increase that number in the next activity?
- Solution = What are you already doing, that your number would be lower if you didn’t do it?
DURING (freezing): Time out!
- Problem = What is not working for you in your ____________?
- Solution = What is going well for you right now in your________ and how can you do more?
BEFORE (frontloading): Before we start this activity, I just want to know…
- Problem = What are some things we might do that would lead to our failure and how can we avoid these individually and as a team?
- Solution = What are some things we might do that would lead to our success and what can we do as individuals and team members to ensure these occur?
FRAMING
Framing refers to the way a challenge or nature immersion experience is introduced to clients by the facilitator. Four kinds of frames or introductions are common:
- Fantasy (uses imaginary playful terms like volcanic eruptions, poison peanut butter, radioactive yoghurt, etc.),
- Reality (uses actual names for objects such as tree, rope, grass, chair, etc.),
- Contextual (describes a metaphor that is general to the category of clientele), and
- Isomorphic (describes a metaphor that is specific to that clientele only and requires their action to mirror their needed growth).
These frameworks are most commonly used in the following program types. However, any frame or introduction can be used in any program type. |
 |
PROGRAM TYPE |
Recreation (FEELING) |
Education (THINKING) |
Development (BEHAVING) |
Therapy (RESISTING) |
FRAMEWORK |
FANTASY |
REALITY |
CONTEXTUAL |
ISOMORPHIC |
Metaphor
A metaphor is an idea, object, or description used in place of a different idea, object, or description to denote comparative similarity between two apparently different things. Three different but related outdoor therapy examples might be:
- the treatment process is much like the expeditionary journey; it is more about the voyage than the destination (adventure/wilderness therapy);
- after a devastating fire, the forest/bush recovers by healing scars and generating new growth, much like therapy (nature-based ecotherapy); and
- resource extraction damage and calls for healing the land are analogous to intergenerational trauma for indigenous people (land-based healing).
In the outdoors, metaphor is a powerful device that enables clients to connect their challenging adventure or nature immersion eco-therapy with their daily lives. The closer the linkages, the more learning transfers, which results in more lasting change. Without metaphor, the two settings (outdoors and daily living) would be so different that transfer would be severely diminished. Metaphor makes meaning of each experience.
The facilitator's job is to apply the aforementioned techniques to strengthen and clarify these connections, thereby enhancing transfer through the conscious use of metaphor. Three methods are most common:
- Spontaneous (during or much later). where clients consider important and relevant connections without assistance from anyone;
- Analogous (after the experience), where clients discover connections through reflective discussions; and
- Structured (before the experience), where experiences are framed or introduced as a contextual message or isomorphic metaphor.
In funnelling (after), clients reflect on metaphors with the question: How was this like life?
In frontloading (before), clients imagine an upcoming metaphor: What will be a moral for this story?
In framing (before), the experience is introduced with a deliberate metaphor that fits the clients loosely (contextual) or precisely (isomorphic).
While the contextual metaphor makes sense at all times to any client in their common category of similar issues, the isomorphic metaphor (same structure) only makes sense to a particular client with unique issues at that moment. The isomorphic introduction tells clients the metaphor in advance and allows them to operate fully within that framework during their experience with the intent that behaviors shown in the experience will emulate those desired in life and thus will bring growth. Obviously, knowing a client extremely well is necessary to create these metaphors.
 |
EXAMPLES OF THE FOUR INTRODUCTIONS (rules and safety concerns are identical).
Fantasy (for children wanting to feel good and have fun): Welcome to Spider's Web. You cannot pass around, under or over, but must go through to safety. To get from this low level floodplain to higher ground before the flood comes, you must pass each other through the spider's web using each opening only once. If you contact the web, the spider bites everyone and you must start over. You have 20 minutes before the flood arrives.
Reality (for analytical adults who over think their issues): The task is to get from this side to that side by passing each other through a unique opening of these strings. Once used, the opening is closed to further use. If anyone touches a string, the group starts over without resetting the clock. You have 20 minutes.
Contextual (for high school teens readying to drop out): Here, we are readying to drop out, but there is your goal of graduation. How can you work together to graduate by passing through the problems of the school year? Obviously, you must take your own unique path with the help of your friends, but once taken, no one can follow you exactly. Be sure not to encounter a problem in the school year that can cause all of you to fail and return everyone back to here and readying to drop out. You have 20 minutes to graduate.
Isomorphic (for store warehouse workers struggling with unethical behavior): Welcome to Distribution Network. This time, you will be shipping goods from your warehouse to my stores through the network. Since my stores are in different locations, you will need to send each shipment through its own unique route. If any shipment is damaged in transit by contacting the network, you will need to voluntarily take it back to the warehouse for repair before shipping again. If any goods arrive at my store damaged, I will return all shipments and we will renegotiate our contract. Delivery deadline is 20 minutes from now. |
The stronger the metaphor, the more likely group discussion is to center on real life problems rather than simply "playing the game."
The PROCESS
Separate from psychotherapy modalities, outdoor therapies typically involve the PROCESS of delivering an activity (see choices below) surrounded by several experiential facilitation steps (see choices above) designed to bring therapeutic benefit to the client in the form of new learning or changes in feeling, thinking, behaving, or resisting. The ten steps are repeated as necessary throughout a program for groups or individuals, preceded by intake sessions and followed by exit interviews. Since the ten steps are repeated, a variation of the Penroses' Eternal Staircase (figured prominently in Esher's illusionary artwork) is used as a model to present these. Each step is explained below this diagram.
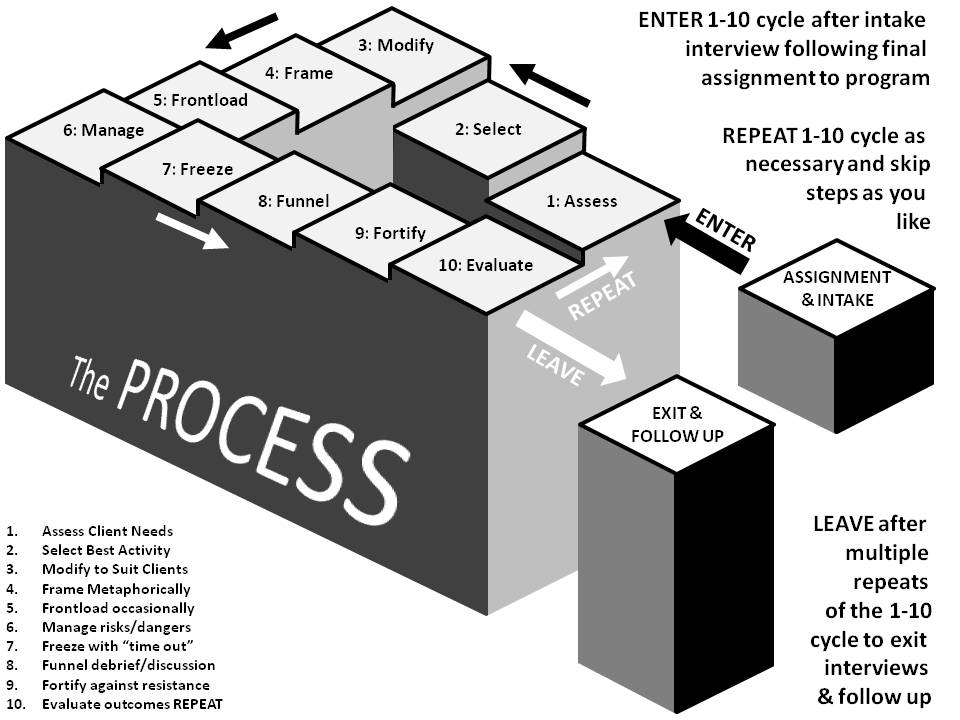
ASSIGNMENT: For pay as they go clients, a voluntary choice is made to enter into therapy. Youth with a criminal background may be court ordered (instead of incarceration or detention). For clients with substance abuse disorder, the decision may be a combination of both involving their families and friends. By whatever means clients arrive at outdoor therapy, their assignment to a program by choice, obligation, or order, begins the PROCESS. During voluntary assignment, the therapist and client discuss what the client seeks, what the therapist offers, and whether these two are likely to fit well together in order to attain what the client seeks. For involuntary assignments, expect some resistance and perhaps not opportunity to discuss. If payment has not already been sorted out, this would be the time to discuss financial matters, before proceeding to the intake session.
INTAKE: During the intake session, the therapist (or a designated facilitator) asks the client(s) a series of health history and symptom questions used to later form an initial working hypothesis. The therapist answers any questions from the client(s) and collects basic information like contact details for the client and another person in case of emergency. Sometimes legal paperwork and medical documents are filled out, especially if these were not completed ahead of intake. The therapist shares important information such as appointment schedules, duration, and ethics, before entering into the PROCESS.
The PROCESS
- ASSESS clients' immediate needs: What is needed next? For groups early in the process, it might be one of the foundational issues such as distrust or miscommunication, but later in the process, this might involve cooperation or resolving conflict. For individuals early in the process, this might be the need to reduce stress and relax, but later in the process, it might include developing confidence or resilience.
- SELECT the best activity to meet those needs: Based on what is needed immediately for a group or individual, the therapist selects an activity from their past experience, the rolodex of ideas they have in memory, and the books or other resources they have available to them. This activity is selected on how well it expects to address the immediate need of the client(s), and allow for valuable learning and change during the debrief discussion, but it may still need modifying.
- MODIFY the activity to custom fit the clients: Beyond structural modifications to match the capabilities of the client(s), the activity may require changing to fit their unique concerns. One common adaptation is to frame that activity with a metaphoric introduction. Early in the process, the metaphor is at least contextual (representing all clients with similar issues). However, at best, and later in the process, the metaphor must be isomorphic (every component, including successful resolution of the activity, must mirror the reality of the client(s) and their needs).
- FRAME the activity with appropriate metaphors: Introduce the activity using the frame created in the previous step. If the metaphor is weak or incorrect in one place, ask the client(s) how they would refer to that place and continue with their strengthened version. Explain the safety concerns for the activity and provide the opportunity to ask clarifying questions. Set a time limit or deadline for completion of the activity.
- FRONTLOAD occasionally: Less than 10% of the time, the therapist or facilitator may want to ask a reflective question before the activity begins in order to adjust the thinking of the client(s) during the activity, where change can be more effective. For example, in a group where they have been committing to change early in the process, but have failed to do so by late in the process, ask a question that reminds them of their commitments. Chances are good that they will behave differently for the first time and the therapist or facilitator can ask them to compare their behaviors during the debrief discussion.
- MANAGE the dangers of the activity underway: During the activity, monitor the client(s) for their adherence to the parameters set out in the introductory frame and observe them for key lessons or notable shifts in feeling, thinking, behaving, or resisting. These will be valuable content for the debrief discussion. If they "break the rules" in order to succeed, simply note this politely and publicly (so it can be discussed in debrief) and then ask them to repeat the activity with more stringent parameters (that potentially block "rule breaking"). Most importantly, remain vigilant around safety and the awareness of dangers.
- FREEZE with a "time out": When they exhibit being "stuck in a rut," stop the action, and ask the client(s) one question. After receiving the answer (or sometimes before, since all the client(s) need to do is think differently), continue the action.
- FUNNEL to debrief or discuss learning and change: After the activity has concluded (due to success, failure, or time expiring), begin the debrief discussion. For a group, gather in a circle. For an individual, walk or sit in isolation away from others and distractions. Apply the facilitation technique (fundamentals or funnelling) and/or psychotherapeutic modality (CBT, DBT, NT, etc.) and gently move the client(s) toward identifying their learning and or making their change.
- FORTIFY against resistance: When faced with resistance apply the fortifying techniques in stepwise sequence.
- EVALUATE outcomes: How did this cycle go? Were the immediate needs of the client(s) met? If so, proceed to the next need. If not, conduct the next cycle with a different activity to address the persistent need. If a new and more critical need arose during the last activity, make this need the center of the next cycle.
REPEAT as necessary: Based on the evaluated outcomes, the therapist (or a facilitator) shifts seamlessly into assessing the clients' immediate needs and repeats the cycle. Evaluation in step 10 feeds assessment in step 1.
EXIT INTERVIEW: When therapy concludes, the client(s) leave the PROCESS and an exit interview is conducted. Sometimes, this is not possible due to circumstances beyond therapist (or facilitator) control. Nevertheless, the exit interview presents the chance to get feedback on the process in specific or therapy in general. How did it go for the client(s)? What did they like/dislike about either? Would they recommend this for a friend? In addition to improving the future performance of the therapist (or a facilitator), the exit interview is a chance to summarize the benefits for the client(s). What was your greatest takeaway? Have your issues been addressed? What do you still need to work on? What are you going to do differently going forward? The exit interview can conclude with the formation of an action plan for groups and individuals.
FOLLOW-UP: Erosive forces work to diminish the impact of therapy. Some clients may relapse or be tempted toward recidivism due to erosive forces. Follow-up involves a number of procedures that can enhance transfer of learning and change, while rendering erosive forces less influential. Follow-up procedures can include regular check-ins, support services in the community, and an occasional return to therapy for one or two sessions with several activities.
ACTIVITIES
A wide variety of activities are used in outdoor therapies. Some of these are described here with accompanying photographic examples.
The initial nature therapy activities must take place outside; these rely on restorative properties and cannot be conducted indoors for their impact.
Sensory Immersion involves fully engaging all of one's senses to become submerged within and part of the surrounding environment.
Listening to forest sounds, watching animals, feeling plants, smelling the soil after rain, and tasting wild edibles are common tactics in sensory immersion. However, we must be careful not to encourage exposing people to harmful fauna or flora such as wasp nests or poisonous vegetation.
Extended movement through an environment (on foot or by bicycle and watercraft) can be considered a sixth sense for the purposes of nature immersion in eco-therapy. |
 |
 |
Yoga & Stretching involves adopting and holding precise body postures (asana) connected by flowing sequences of movement (vinyasa) to understand and enlighten one's physical and mental self. It becomes a spiritual discipline, fully uniting mind, body, and soul in harmony, through meditation and contemplation during practice. This can be followed by relaxation exercises.
Chanting and breathing exercises can be added for greater control and spiritual unification. As a life approach to healthy living, it is often combined with nutritious food and plentiful exercise. For those who are not use to exercise outdoors, it can be a valuable warmup. |
Meditation & Contemplation are mindful focused concentrations on an object, thought, or activity to train attention and awareness. A cognitively clear and emotionally calmed state can be achieved by mindful concentration on something found in nature.
This state can enhanced by "earthing" or "grounding" oneself to the electronically charged planet, by touching rock or soil with bare feet or hands.
Meditation or contemplation followed by personal reflection (through journaling or expressive artwork) adds to the understanding and meaning of attention and awareness. |
 |
 |
Ecological Exercises are sometimes used to deeply immerse participants in restorative nature and to utilize their senses under the guise of science. By closely examining nature from a scientific perspective, the resistant and analytical thinker slowly begins to warm up to the idea of nature-based eco-therapy. Expressive arts can also be used similarly for the resistant, but creative thinker.
While the following adventure therapy activities may take place outside, these do not rely on nature for their impact and so many could be conducted indoors. |
Socialization games are playful activities used to put people at ease. They serve several other functions.
Warmups get people to raise their heart rates and loosen up their stiff muscles before the activities that follow. Openers set a tone for therapy and introduce people to each other.
Socializers deinhibit and allow people to get to know one another. Energizers invigorate and raise enthusiasm levels when needed.
Fillers occupy downtime or program gaps by consuming time with fun and a riddle or puzzle. Closers end the sessions by highlighting lessons learned, celebrating achievements gained, and bringing commitments for future change. |
 |
 |
Group Initiatives invite groups to solve unusual problems. In a typical program, these focus on team-building (through trust, communication, cooperation, and more), but can also be adapted to become more individually focused (on developing self-efficacy, confidence, resilience, and more) by separating group members and giving individual isolated tasks to accomplish.
These problem-solving initiatives can be divided into tools of teamwork, where only one component is addressed at one time (such as trust falls) or into tests of teamwork, where multiple components are necessary to successfully plan, communicate, and execute solutions to the problems (such as the spider's web above). |
Ropes/Challenge Courses are a series of obstacles (elements) that are constructed between trees, utility poles, or steel towers. Participants take turns navigating through the course by overcoming each obstacle or crossing each element.
The elements can be constructed at ground level or at great heights above ground. Low elements, at ground level, are protected by fellow group members spotting to physically support a participant. High elements, several meters above ground, are protected by a safety line. The safety line can have a fixed length, providing for a short fall, or be connected to others on the ground, who "belay" the participant and can lower him/her when tired.
An individually focused activity (using risk taking to develop self-efficacy, confidence, resilience, and more) can be adapted to achieve team-building (through trust, communication, cooperation, and more) by modifying an element for 2+ participants at a time, who may or may not be tied together in some way. |
 |
 |
Outdoor Pursuits are human-powered activities such as hiking, backpacking, watercraft paddling (flat water, open ocean, or whitewater), bicycling (touring or mountain), surfing, rock climbing, mountaineering, skiing, snowshoeing, spelunking (caving), sailing, etc. They do not include motorized (snowmobiling, motorcycling, and 4x4 off-roading) or animal powered (horse riding or dog sledding) forms of outdoor recreation.
Outdoor pursuits can be based in one place for a few days or travel to remote locations on a multi-day overnight expedition. The purpose of these activities is not necessarily to learn new skills (although this happens), but are more about creating opportunities for risk taking (to develop the intrapersonal self) and conflict resolution or group dynamics (to develop pro-social skills and the interpersonal self). This category is dependent on the outdoors, although some activities can take place indoors with artificial environs (like an indoor climbing wall). |
Simulations take place with technologies or board games. These are imitations of real-world processes or systems and can range from building and managing a fictional community or project, through role playing a surgeon or ecosystem, to the virtual reality of sailing a tall ship or piloting a spacecraft.
In these versions, participants create an avatar (artificial life form or player piece) to represent themselves and they move their avatars through the simulation encountering and addressing task or relationship challenges along the way that require problem-solving and decision-making skills.
Ethically, violent and popular combat video games or first-person shooter simulations are excluded from this category for obvious reasons. |
 |
The combination of both nature and adventure activities is common in more remote outdoor therapy programs.
|
|